Obstruted Defaecation Web
| Classification of Internal Rectal Intussusception |
|
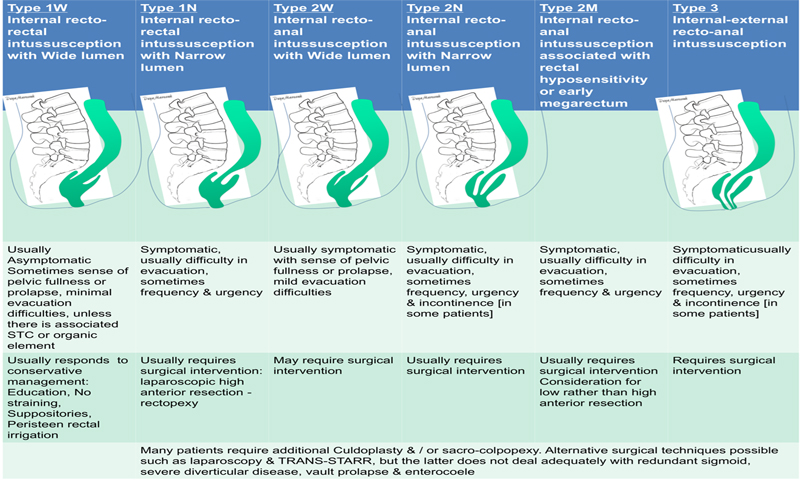
Introduction A clinically useful classification of rectal wall abnormalities is currently lacking. Coloproctologists need to come to a consensus regarding a new classification of these abnormalities that can distinguish subtypes and be useful in choice of treatment in symptomatic patients. I ouline below my own classification [which remains a dynamic work in progress]. This can be viewed as a proposal & may eventually serve as the basis of a more universally agreed classification. Currently internal rectal intussusception is classified into recto-rectal [high] & recto-anal [low] subtypes, normally based on the height of intussusception from the anal canal on proctography. Few clinicians classify intussusception, based on digital rectal examination [I am one of them]. Over the years, based on observation of the many patients I treated with OBD, I came to realize the importance of several other factors in addition to the height of the intussusception above the anal canal. Among the most important other factors is the diameter of the intussuscepted bowel, presence of rectal hyposensitivity & presence of associated secondary delayed colonic transit. Based on these I proposed the following anatomico-functional classification based on these clinical, physiologic & prographic findings:
IRI Anatomico-Functional Classification Type 1: Internal recto-rectal intussusception
Type 2: Internal recto-anal intussusception
Type 3: Internal-external recto-anal intussusception
It seems from our experience that intussusception with wide internal lumen is less likely to cause obstructed defaecatory symptoms, at least not severe, but may equally be associated with sense of prolapse or deep seated discomfort in pelvis. Presence of left sided slow transit favours more bowel resection, while rectal hyposensitivity may favour a more lower resection. What defines a wide or a narrow lumen is currently subjective, based on digital rectal examination. Presence of delayed transit or rectal hyposensitivity on ano-rectal physiology should be interpreted with caution and in the clinical context of individual patients. Finally, since S shaped rectum can on occasions cause as much difficulty in evacuation as internal rectal intussusception, a future classification may take this as well as rectocoele into account. |