Obstruted Defaecation Web
| Rectocoele |
|
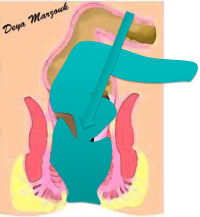
Rectocoele is a term used to describe abnormal bulge of rectal wall, mostly to the front, bulging into the vagina. It can be thought of as a is a hernia of the anterior wall of the rectum into the lumen of the vagina. Rarely rectocoeles can be posterior or lateral Rectoceles result from damage to the rectovaginal septum, mostly from child delivery. It may take the form of an isolated defect in the rectovaginal septum or attenuation and thinning of the rectovaginal septum. Rectocoeles are often associated with internal rectal intussusception & perineal body defects. Rectocoeles may be classified as low, mid or high depending on their height in the posterior vaginal wall. A more clinically relevant classification would be simply divide rectocoeles to small asymptomatic & large symptomatic. Symptoms generally fall into one or more of four categories. These include 1) the sensation of a bulging lump in the vagina as well as sensation of perineal or pelvic pressure, 2) obstructed defaecation symptoms including incomplete evacuation and in particular patient may report the need to use fingers to support the vagina or perineum during defaecation. 3) Some patients will complain of faecal incontinence, which is particularly pronounced post defaecation. 4) Some ladies also have a feeling of vaginal laxity during sexual intercourse and occasionally a sense of vaginal blockage for their partners. Some may have leakage during intercourse.
Rectocoele is easy to detect during digital rectal examination with the index pushing forward into the vagina. Larger rectocoeles may be visible on straining. Digital rectal examination is vital to differentiate a low enterocoele from rectocoele. Defaecating proctography is useful in assessing the significance of rectocoele to defaecatory symptoms Rectocoeles were thought to be an important cause of obstructed defaecation, but currently I believe that only really big rectocoele cause defaecatory difficulties. Rectocoeles on the other hand are important cause of feeling of incomplete evacuation & post defaecation leakage. Rectocoeles can be repaired transvaginally, transrectally, using a transperineal approach [usually including an anterior levatorplasty as well] or laparoscopically as part of resection-rectopexy. It is important not to have rectocoeles repaired in isolation in patients with bowel or defaecation symptoms as the resulting fibrosis in the rectovaginal septum makes full mobilization to reduce the internal rectal intussusception more difficult & increases the risk of rectal damage during the procedure. I now believe that rectocoeles are probably best fixed by pulling the rectal wall up, along with the internal rectal intussusception, normally as a part resection-rectopexy. Alternatively, they can be repaired with the intussusception using a trans-STARR procedure. Repair of rectocoeles in isolation is only justified when there no concomitant bowel symptoms |